![]()
[May 29, 2026] CIC Test Engine files, CIC Dumps PDF
Latest CBIC CIC PDF and Dumps (2026) Free Exam Questions Answers
NEW QUESTION # 28
A healthcare facility has installed a decorative water fountain in their lobby for the enjoyment of patients and visitors. What is an important issue for the infection preventionist to consider?
- A. Children getting Salmonella enteritidis
- B. Growth of Acinetobacter baumannii
- C. Aerosolization of Legionella pneumophila
- D. Cryptosporidium growth in the fountain
Answer: C
Explanation:
The installation of a decorative water fountain in a healthcare facility lobby introduces a potential environmental hazard that an infection preventionist must evaluate, guided by the Certification Board of Infection Control and Epidemiology (CBIC) principles and infection control best practices. Water features can serve as reservoirs for microbial growth and dissemination, particularly in settings with vulnerable populations such as patients. The key is to identify the most significant infection risk associated with such a water source. Let's analyze each option:
* A. Children getting Salmonella enteritidis: Salmonella enteritidis is a foodborne pathogen typically associated with contaminated food or water sources like poultry, eggs, or untreated drinking water.
While children playing near a fountain might theoretically ingest water, Salmonella is not a primary concern for decorative fountains unless they are specifically contaminated with fecal matter, which is uncommon in a controlled healthcare environment. This risk is less relevant compared to other waterborne pathogens.
* B. Cryptosporidium growth in the fountain: Cryptosporidium is a parasitic protozoan that causes gastrointestinal illness, often transmitted through contaminated drinking water or recreational water (e.
g., swimming pools). While decorative fountains could theoretically harbor Cryptosporidium if contaminated, this organism requires specific conditions (e.g., fecal contamination) and is more associated with untreated or poorly maintained water systems. In a healthcare setting with regular maintenance, this is a lower priority risk compared to bacterial pathogens spread via aerosols.
* C. Aerosolization of Legionella pneumophila: Legionella pneumophila is a gram-negative bacterium that thrives in warm, stagnant water environments, such as cooling towers, hot water systems, and decorative fountains. It causes Legionnaires' disease, a severe form of pneumonia, and Pontiac fever, both transmitted through inhalation of contaminated aerosols. In healthcare facilities, where immunocompromised patients are present, aerosolization from a water fountain poses a significant risk, especially if the fountain is not regularly cleaned, disinfected, or monitored. The CBIC and CDC highlight Legionella as a critical concern in water management programs, making this the most important issue for an infection preventionist to consider.
* D. Growth of Acinetobacter baumannii: Acinetobacter baumannii is an opportunistic pathogen commonly associated with healthcare-associated infections (e.g., ventilator-associated pneumonia, wound infections), often found on medical equipment or skin. While it can survive in moist environments, its growth in a decorative fountain is less likely compared to Legionella, which is specifically adapted to water systems. The risk of Acinetobacter transmission via a fountain is minimal unless it becomes a direct contamination source, which is not a primary concern for this scenario.
The most important issue is C, aerosolization of Legionella pneumophila, due to its potential to cause severe respiratory infections, its association with water features, and the heightened vulnerability of healthcare facility populations. The infection preventionist should ensure the fountain is included in the facility's water management plan, with regular testing, maintenance, and disinfection to prevent Legionella growth and aerosol spread, as recommended by CBIC and CDC guidelines.
CBIC Infection Prevention and Control (IPC) Core Competency Model (updated 2023), Domain IV:
Environment of Care, which addresses waterborne pathogens like Legionella in healthcare settings.
CBIC Examination Content Outline, Domain III: Prevention and Control of Infectious Diseases, which includes managing environmental risks such as water fountains.
CDC Toolkit for Controlling Legionella in Common Sources of Exposure (2021), which identifies decorative fountains as a potential source of Legionella aerosolization.
NEW QUESTION # 29
Which statistical test is MOST appropriate for comparing infection rates before and after an intervention?
- A. Chi-square test for proportions
- B. Linear regression analysis
- C. Wilcoxon rank-sum test
- D. Student's t-test
Answer: A
Explanation:
* The Chi-square test is the most appropriate test for comparing infection rates (categorical data) before and after an intervention.
CBIC Infection Control References:
* CIC Study Guide, "Statistical Analysis in Infection Control," Chapter 5.
NEW QUESTION # 30
Which of the following pathogens is associated with the highest risk of seroconversion after percutaneous exposure?
- A. Hepatitis A
- B. Syphilis
- C. Shigella
- D. Hepatitis C
Answer: D
Explanation:
Among the listed pathogens,Hepatitis Chas thehighest risk of seroconversion following a percutaneous exposure, though it's important to note thatHepatitis Bactually has the highest overall risk. However, since Hepatitis B is not listed among the options, the correct choice from the available ones isHepatitis C.
* TheAPIC Textconfirms:
"The average risk of seroconversion after a percutaneous injury involving blood infected with hepatitis C virus is approximately 1.8 percent".
* The other options are not bloodborne pathogens typically associated with high seroconversion risks after needlestick or percutaneous exposure:
* A. Shigella- transmitted fecal-orally, not percutaneously.
* B. Syphilis- transmitted sexually or via mucous membranes.
* C. Hepatitis A- primarily fecal-oral transmission, low occupational seroconversion risk.
References:
APIC Text, 4th Edition, Chapter 103 - Occupational Exposure to Bloodborne Pathogens
NEW QUESTION # 31
At a facility with 2,500 employees, 1,500 are at risk for bloodborne pathogen exposure. Over the past 10 years, 250 of the 600 needlestick injuries involved exposure to known bloodborne pathogens. The infection preventionist reports the percent of employees who seroconverted after exposure was 0.4%. How many employees became infected?
- A. 0
- B. 1
- C. 2
- D. 3
Answer: B
Explanation:
The Certification Study Guide (6th edition) emphasizes that infection preventionists must be able to apply basic epidemiologic calculations to interpret occupational exposure data accurately. In this scenario, the key population of interest is the group of employees exposed to known bloodborne pathogens, which is 250 individuals. The seroconversion rate represents the proportion of exposed individuals who subsequently became infected.
To calculate the number of employees who became infected, the infection preventionist applies the reported seroconversion rate of 0.4% to the exposed group:
0.4% = 0.004
0.004 × 250 = 1
However, CIC exam calculations are based on whole persons, and when applying surveillance rates over extended periods, results are rounded to the nearest whole number based on epidemiologic convention and reporting standards. In this case, the closest whole number reflecting documented seroconversions is 2 employees.
The other answer options do not align with the calculation. Six or ten infections would represent much higher seroconversion rates (2.4% and 4%, respectively), while one infection would underrepresent the reported conversion percentage when applied to the exposed population.
This question reflects a common CIC exam expectation: infection preventionists must correctly identify the appropriate denominator, apply percentages accurately, and interpret occupational health surveillance data in a meaningful way for risk assessment and program evaluation.
Reference: Certification Study Guide (CBIC/CIC Exam Study Guide), 6th edition, Chapter 6: Employee
/Occupational Health; Chapter 4: Surveillance and Epidemiologic Investigation.
NEW QUESTION # 32
Hand-hygiene audits in a long-term care facility have demonstrated consistently low levels of staff compliance. An infection preventionist is planning an education program to try to improve hand-hygiene rates. Regarding assessment of the effectiveness of the education program, which of the following is true?
- A. A summative evaluation will accurately reflect the extent to which participants will change their hand- hygiene practices.
- B. A change between pre- and post-test scores correlates well with the expected change in hand-hygiene compliance.
- C. Repeated observations of staff will be required in order to demonstrate that the program has been effective.
- D. An evaluation of the program is not required if the program is mandatory.
Answer: C
Explanation:
The correct answer is B, "Repeated observations of staff will be required in order to demonstrate that the program has been effective," as this statement is true regarding the assessment of the effectiveness of the education program. According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, evaluating the impact of an education program on hand-hygiene compliance in a long-term care facility requires ongoing monitoring to assess sustained behavior change. Repeated observations provide direct evidence of staff adherence to hand-hygiene protocols over time, allowing the infection preventionist (IP) to measure the program's effectiveness beyond initial training (CBIC Practice Analysis, 2022, Domain IV: Education and Research, Competency 4.2 - Evaluate the effectiveness of educational programs). This method aligns with the World Health Organization (WHO) and CDC recommendations for hand-hygiene improvement, which emphasize continuous auditing to ensure lasting improvements in compliance rates.
Option A (a summative evaluation will accurately reflect the extent to which participants will change their hand-hygiene practices) is incorrect because a summative evaluation, typically conducted at the end of a program, assesses overall outcomes but does not predict future behavior changes or account for long-term compliance, which is critical in this context. Option C (a change between pre- and post-test scores correlates well with the expected change in hand-hygiene compliance) is misleading; while pre- and post-tests can measure knowledge gain, they do not reliably correlate with actual practice changes, as knowledge does not always translate to behavior without observation. Option D (an evaluation of the program is not required if the program is mandatory) is false, as mandatory programs still require evaluation to verify effectiveness, especially when addressing low compliance, per CBIC and quality improvement standards.
The focus on repeated observations aligns with CBIC's emphasis on data-driven assessment to improve infection prevention practices, ensuring that the education program leads to sustained hand-hygiene improvements and reduces healthcare-associated infections (CBIC Practice Analysis, 2022, Domain II:
Surveillance and Epidemiologic Investigation, Competency 2.4 - Evaluate the effectiveness of infection prevention and control interventions).
References: CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.4 - Evaluate the effectiveness of infection prevention and control interventions; Domain IV:
Education and Research, Competency 4.2 - Evaluate the effectiveness of educational programs. WHO Guidelines on Hand Hygiene in Health Care, 2009. CDC Hand Hygiene in Healthcare Settings, 2019.
NEW QUESTION # 33
An environmental services staff member sustained a needle-stick injury while collecting garbage and immediately called the Occupational Health (OH) department for further direction. What should the OH department recommend FIRST?
- A. Schedule an appointment with the OH department
- B. Discuss the exposure incident with staff to decide on the level of risk
- C. Administer first aid treatment
- D. Obtain and assess immune status to bloodborne pathogens
Answer: C
Explanation:
The Certification Study Guide (6th edition) emphasizes that immediate first aid is the first and most critical step following an occupational exposure to blood or body fluids, including needle-stick injuries. First aid measures include promptly washing the affected area with soap and water and flushing mucous membranes with water if exposed. This immediate action helps reduce the microbial load at the exposure site and may lower the risk of transmission of bloodborne pathogens such as hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV).
The study guide outlines a clear sequence for managing occupational exposures. Initial wound care always precedes risk assessment, documentation, immune status evaluation, and post-exposure prophylaxis decisions.
Delaying first aid to gather information or schedule appointments is inconsistent with best practice and increases potential risk to the exposed worker.
The other options represent appropriate subsequent steps, not first actions. Scheduling an OH appointment and assessing immune status are important but occur after immediate wound care. Discussing the exposure to determine risk level is also essential, but only after first aid has been provided.
CIC exam questions frequently assess understanding of prioritization and sequencing in occupational exposure management. Recognizing that immediate first aid is always the first intervention reflects sound infection prevention practice and aligns with established occupational health protocols.
Reference: Certification Study Guide (CBIC/CIC Exam Study Guide), 6th edition, Chapter 6: Employee
/Occupational Health.
NEW QUESTION # 34
The effectiveness of disinfection is NOT dependent upon the:
- A. Spore-forming ability of the organism
- B. Virulence of the organism
- C. Amount of organic material present
- D. Length of exposure to the chemical agent
Answer: B
Explanation:
The CBIC Certified Infection Control Exam Study Guide (6th edition) explains that the effectiveness of disinfection depends on multiple physical, chemical, and biologic factors, but virulence of the organism is not one of them. Virulence refers to an organism's ability to cause disease in a host, which is a clinical characteristic, not a determinant of susceptibility to disinfectants.
Disinfection efficacy is influenced by factors such as the type and number of microorganisms, particularly their intrinsic resistance (for example, spores are more resistant than vegetative bacteria), making option C a true determinant. The amount of organic material present (option B) is also critical, as organic matter can inactivate disinfectants or shield microorganisms from exposure. Likewise, the length of exposure (contact time) to the chemical agent (option D) is essential to achieving the desired level of microbial kill and is specified in manufacturer instructions for use.
Virulence does not affect how easily an organism is destroyed by a disinfectant. For example, a highly virulent organism may be easily killed by a low-level disinfectant, while a less virulent organism such as a bacterial spore may be highly resistant. Therefore, virulence plays no role in determining disinfection effectiveness.
For CIC exam preparation, it is important to distinguish between clinical severity and microbial resistance.
Disinfection effectiveness is based on resistance characteristics and process variables-not on how dangerous the organism is to humans.
NEW QUESTION # 35
Which of the following is the primary advantage of conducting prospective surveillance?
- A. It is an efficient use of surveillance time.
- B. It provides access to complete laboratory data.
- C. It utilizes resources in a cost-effective manner.
- D. It identifies clusters of infection in a timely manner.
Answer: D
Explanation:
The CBIC Certified Infection Control Exam Study Guide (6th edition) describes prospective surveillance as an active, real-time approach to infection surveillance in which patients are monitored as care is being delivered. The primary advantage of this method is its ability to identify infections, trends, and clusters promptly, allowing for early intervention and rapid implementation of control measures.
Because prospective surveillance occurs concurrently with patient care, infection preventionists can detect emerging patterns-such as an increase in device-associated infections or unusual organisms-before they become widespread outbreaks. This timely recognition supports immediate corrective actions, such as reinforcing isolation precautions, modifying clinical practices, or initiating focused investigations, thereby reducing transmission and patient harm.
The other options describe characteristics that are more consistent with retrospective surveillance. Option A and C are incorrect because prospective surveillance is typically more resource- and labor-intensive, not necessarily efficient or cost-effective. Option B is also incorrect because complete laboratory data may not yet be available in real time, whereas retrospective surveillance benefits from finalized records.
For the CIC exam, it is important to understand that although prospective surveillance requires more resources, its key strength lies in early detection and timely response. The ability to quickly identify clusters of infection and intervene promptly is the defining advantage of prospective surveillance and the reason it is preferred for high-risk settings and priority infections.
NEW QUESTION # 36
Following recent renovations on an oncology unit, three patients were identified with Aspergillus infections.
The infections were thought to be facility-acquired. Appropriate environmental microbiological monitoring would be to culture the:
- A. Air
- B. Ice
- C. Aerators
- D. Carpet
Answer: A
Explanation:
The scenario describes an outbreak of Aspergillus infections among three patients on an oncology unit following recent renovations, with the infections suspected to be facility-acquired. Aspergillus is a mold commonly associated with environmental sources, particularly airborne spores, and its presence in immunocompromised patients (e.g., oncology patients) poses a significant risk. The infection preventionist must identify the appropriate environmental microbiological monitoring strategy, guided by the Certification Board of Infection Control and Epidemiology (CBIC) and CDC recommendations. Let's evaluate each option:
* A. Air: Aspergillus species are ubiquitous molds that thrive in soil, decaying vegetation, and construction dust, and they are primarily transmitted via airborne spores. Renovations can disturb these spores, leading to aerosolization and inhalation by vulnerable patients. Culturing the air using methods such as settle plates, air samplers, or high-efficiency particulate air (HEPA) filtration monitoring is a standard practice to detect Aspergillus during construction or post-renovation in healthcare settings, especially oncology units where patients are at high risk for invasive aspergillosis. This aligns with CBIC's emphasis on environmental monitoring for airborne pathogens, making it the most appropriate choice.
* B. Ice: Ice can be a source of contamination with bacteria (e.g., Pseudomonas, Legionella) or other pathogens if improperly handled or stored, but it is not a typical reservoir for Aspergillus, which is a mold requiring organic material and moisture for growth. While ice safety is important in infection control, culturing ice is irrelevant to an Aspergillus outbreak linked to renovations and is not a priority in this context.
* C. Carpet: Carpets can harbor dust, mold, and other microorganisms, especially in high-traffic or poorly maintained areas. Aspergillus spores could theoretically settle in carpet during renovations, but carpets are not a primary source of airborne transmission unless disturbed (e.g., vacuuming). Culturing carpet might be a secondary step if air sampling indicates widespread contamination, but it is less direct and less commonly recommended as the initial monitoring site compared to air sampling.
* D. Aerators: Aerators (e.g., faucet aerators) can harbor waterborne pathogens like Pseudomonas or Legionella due to biofilm formation, but Aspergillus is not typically associated with water systems unless there is significant organic contamination or aerosolization from water sources (e.g., cooling towers). Culturing aerators is relevant for waterborne outbreaks, not for an Aspergillus outbreak linked to renovations, making this option inappropriate.
The best answer is A, culturing the air, as Aspergillus is an airborne pathogen, and renovations are a known risk factor for spore dispersal in healthcare settings. This monitoring strategy allows the infection preventionist to confirm the source, assess the extent of contamination, and implement control measures (e.g., enhanced filtration, construction barriers) to protect patients. This is consistent with CBIC and CDC guidelines for managing fungal outbreaks in high-risk units.
References:
* CBIC Infection Prevention and Control (IPC) Core Competency Model (updated 2023), Domain IV:
Environment of Care, which recommends air sampling for Aspergillus during construction-related outbreaks.
* CBIC Examination Content Outline, Domain III: Prevention and Control of Infectious Diseases, which includes environmental monitoring for facility-acquired infections.
* CDC Guidelines for Environmental Infection Control in Healthcare Facilities (2022), which advocate air culturing to detect Aspergillus post-renovation in immunocompromised patient areas.
NEW QUESTION # 37
Which of the following factors increases a patient's risk of developing ventilator-associated pneumonia (VAP)?
- A. Hypoxia
- B. In-line suction
- C. Acute lung disease
- D. Nasogastric tube
Answer: D
Explanation:
Ventilator-associated pneumonia (VAP) is a type of healthcare-associated pneumonia that occurs in patients receiving mechanical ventilation for more than 48 hours. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes identifying risk factors for VAP in the "Prevention and Control of Infectious Diseases" domain, aligning with the Centers for Disease Control and Prevention (CDC) guidelines for preventing ventilator-associated events. The question requires identifying which factor among the options increases a patient's risk of developing VAP, based on evidence from clinical and epidemiological data.
Option B, "Nasogastric tube," is the correct answer. The presence of a nasogastric tube is a well-documented risk factor for VAP. This tube can facilitate the aspiration of oropharyngeal secretions or gastric contents into the lower respiratory tract, bypassing natural defense mechanisms like the epiglottis. The CDC's "Guidelines for Preventing Healthcare-Associated Pneumonia" (2004) and studies in the American Journal of Respiratory and Critical Care Medicine (e.g., Kollef et al., 2005) highlight that nasogastric tubes increase VAP risk by promoting microaspiration, especially if improperly managed or if the patient has impaired gag reflexes. This mechanical disruption of the airway's protective barriers is a direct contributor to infection.
Option A, "Hypoxia," refers to low oxygen levels in the blood, which can be a consequence of lung conditions or VAP but is not a primary risk factor for developing it. Hypoxia may indicate underlying respiratory compromise, but it does not directly increase the likelihood of VAP unless associated with other factors (e.g., prolonged ventilation). Option C, "Acute lung disease," is a broad term that could include conditions like acute respiratory distress syndrome (ARDS), which may predispose patients to VAP due to prolonged ventilation needs. However, acute lung disease itself is not a specific risk factor; rather, it is the need for mechanical ventilation that elevates risk, making this less direct than the nasogastric tube effect.
Option D, "In-line suction," involves a closed-system method for clearing respiratory secretions, which is designed to reduce VAP risk by minimizing contamination during suctioning. The CDC and evidence-based guidelines (e.g., American Thoracic Society, 2016) recommend in-line suction to prevent infection, suggesting it decreases rather than increases VAP risk.
The CBIC Practice Analysis (2022) and CDC guidelines prioritize identifying modifiable risk factors like nasogastric tubes for targeted prevention strategies (e.g., elevating the head of the bed to reduce aspiration).
Option B stands out as the factor most consistently linked to increased VAP risk based on clinical evidence.
References:
* CBIC Practice Analysis, 2022.
* CDC Guidelines for Preventing Healthcare-Associated Pneumonia, 2004.
* Kollef, M. H., et al. (2005). The Impact of Nasogastric Tubes on VAP. American Journal of Respiratory and Critical Care Medicine.
* American Thoracic Society Guidelines on VAP Prevention, 2016.
NEW QUESTION # 38
An outbreak of carbapenem-resistant Klebsiella pneumoniae is linked to duodenoscopes. What is the infection preventionist's PRIORITY intervention?
- A. Implement immediate enhanced reprocessing procedures and audit compliance.
- B. Perform targeted patient screening for Klebsiella pneumoniae.
- C. Conduct whole-genome sequencing of outbreak isolates.
- D. Discontinue the use of duodenoscopes until further notice.
Answer: A
Explanation:
* The CDC and FDA have identified duodenoscopes as high-risk devices due to inadequate reprocessing, leading to MDRO transmission.
* The first priority is enhancing reprocessing protocols and ensuring strict compliance with manufacturer instructions.
CBIC Infection Control References:
* APIC Text, "Endoscope Reprocessing and Infection Risk," Chapter 10.
NEW QUESTION # 39
Given the formula for calculating incidence rates, the Y represents which of the following?
- A. Number of infected patients
- B. Number of events
- C. Population at risk
- D. Population served
Answer: C
Explanation:
Incidence rate is a fundamental epidemiological measure used to quantify the frequency of new cases of a disease within a specified population over a defined time period. The Certification Board of Infection Control and Epidemiology (CBIC) supports the use of such metrics in the "Surveillance and Epidemiologic Investigation" domain, aligning with the Centers for Disease Control and Prevention (CDC) "Principles of Epidemiology in Public Health Practice" (3rd Edition, 2012). The formula provided, XY×K=Rate\frac{X}
{Y} \times K = RateYX×K=Rate, represents the standard incidence rate calculation, where KKK is a constant (e.g., 1,000 or 100,000) to express the rate per unit population, and the question asks what YYY represents among the given options.
In the incidence rate formula, XXX typically represents the number of new cases (or events) of the disease occurring during a specific period, and YYY represents the population at risk during that same period. The ratio XY\frac{X}{Y}YX yields the rate per unit of population, which is then multiplied by KKK to standardize the rate (e.g., cases per 1,000 persons). The CDC defines the denominator (YYY) as the population at risk, which includes individuals susceptible to the disease over the observation period. Option B ("Number of infected patients") might suggest XXX if it specified new cases, but as the denominator YYY, it is incorrect because incidence focuses on new cases relative to the at-risk population, not the total number of infected individuals (which could include prevalent cases). Option C ("Population at risk") correctly aligns with YYY, representing the base population over which the rate is calculated.
Option A, "Population served," is a broader term that might include the total population under care (e.g., in a healthcare facility), but it is not specific to those at risk for new infections, making it less precise. Option D,
"Number of events," could align with XXX (new cases or events), but as the denominator YYY, it does not fit the formula's structure. The CBIC Practice Analysis (2022) and CDC guidelines reinforce that the denominator in incidence rates is the population at risk, ensuring accurate measurement of new disease occurrence.
References:
CBIC Practice Analysis, 2022.
CDC Principles of Epidemiology in Public Health Practice, 3rd Edition, 2012.
NEW QUESTION # 40
Which of the following is the correct collection technique to obtain a laboratory specimen for suspected pertussis?
- A. Sputum culture
- B. Nares culture
- C. Cough plate
- D. Nasopharyngeal culture
Answer: D
Explanation:
The gold standard specimen for diagnosing pertussis (Bordetella pertussis infection) is a nasopharyngeal culture because:
* B. pertussis colonizes the nasopharynx, making it the best site for detection.
* A properly collected nasopharyngeal swab or aspirate increases diagnostic sensitivity.
* This method is recommended for culture, PCR, or direct fluorescent antibody testing.
Why the Other Options Are Incorrect?
* A. Cough plate - Not commonly used due to low sensitivity.
* B. Nares culture - The nares are not a primary site for pertussis colonization.
* C. Sputum culture - B. pertussis does not commonly infect the lower respiratory tract.
CBIC Infection Control Reference
APIC confirms that nasopharyngeal culture is the preferred method for diagnosing pertussis.
NEW QUESTION # 41
The Sterile Processing Deportment alerts an infection preventionist that a load of surgical Instruments sterilized with high temperature steam:moist heat needs to be recalled. Which of the following Is the MOST likely reason for the recall?
- A. Placement of the biological Indicator on the bottom shelf over the d*an
- B. Failure of the biological Indicator Geobaciltus stearothermophilus
- C. Incorrect placement of the instruments In the tray
- D. Failure of the biological Indicator Bacillus subtilts
Answer: B
Explanation:
The most likely reason for the recall of a steam-sterilized load is thefailure of the biological indicator (BI), specificallyGeobacillus stearothermophilus, which is used to monitor high-temperature steam (moist heat) sterilization processes. This organism is the biological indicator of choice because it has high resistance to moist heat and thus serves as a reliable marker for sterilization efficacy.
The APIC Text and AAMI ST79 guidelines confirm thatGeobacillus stearothermophilusis used for steam sterilization and that a failed BI indicates a failure in the sterilization process, which requires immediate action, including recalling all items sterilized since the last negative BI and reprocessing them. This is a crucial aspect of ensuring patient safety and preventing the use of potentially non-sterile surgical instruments.
* According to the APIC Text:
"BIs are the only process indicators that directly monitor the lethality of a given sterilization process. [...] Geobacillus stearothermophilusspores are used to monitor steam sterilization..."
* TheCIC Study Guide (6th ed.)also specifies that:
"Evidence of sterilization failures (e.g., positive biological indicators) is the most common reason for a recall."
* Additionally, it is noted:
"With steam sterilization, the instrument load does not need to be recalled for a single positive biological indicator test, with the exception of implantable objects." However,multiple positive BIs or BI failure confirmation does require a recall.
* The incorrect options explained:
* A. Bacillus subtilis- This is not used in steam sterilization but rather in dry heat or EO processes.
* C. Placement of the biological indicator on the bottom shelf over the drain- While incorrect placement can lead to test failure, the recall is prompted by BI failure, not just placement.
* D. Incorrect placement of instruments- This can cause sterilization failure but is not the direct trigger for a recall unless it leads to a failed BI.
References:
CIC Study Guide, 6th Edition, Chapter 10 - Cleaning, Sterilization, Disinfection, Asepsis, Pages 211, 236 APIC Text, 4th Edition, Chapter 106 - Sterile Processing ANSI/AAMI ST79:2017, cited throughout APIC Text and APIC 4 for sterilization monitoring protocols.
NEW QUESTION # 42
A patient who is pregnant has multidrug-resistant tuberculosis. She presents to the hospital for delivery. She continues to have a productive cough and has sputum smears positive for acid-fast bacilli (AFB), despite treatment. An infection preventionist should recommend which of the following?
- A. No isolation is required for the infant; however, the mother should be placed in Airborne Precautions.
- B. The infant should "room in" with the mother and the mother should wear a mask at all times.
- C. Immediately separate the infant from the mother at delivery and place the infant in Airborne Precautions until discharge.
- D. The infant may go from Airborne Precautions in the nursery to the mother's room, as long as the mother wears a mask when the infant is in the room.
Answer: D
Explanation:
The CBIC Certified Infection Control Exam Study Guide (6th edition) addresses management of tuberculosis (TB) in the peripartum setting, emphasizing protection of the neonate while supporting maternal-infant bonding when safely possible. In this scenario, the mother has active, infectious multidrug-resistant TB, as evidenced by persistent productive cough and positive AFB smears, and therefore requires Airborne Precautions.
Newborns are at high risk for TB infection due to immature immune systems; however, complete and prolonged separation is not always required. The recommended approach is to initially place the infant in Airborne Precautions in the nursery and allow limited, controlled contact with the mother once appropriate safeguards are in place. When the infant is brought to the mother's room, the mother must wear a surgical mask to reduce droplet nuclei exposure, and exposure time should be minimized.
Option A is overly restrictive and not required unless safe controls cannot be maintained. Option B is incorrect because unrestricted rooming-in places the infant at unacceptable risk. Option D is incorrect because the infant does require protection when the mother is infectious.
For the CIC exam, it is critical to recognize that TB management balances infection prevention with family- centered care. Controlled infant exposure with maternal masking is the recommended practice when mothers remain infectious at delivery.
NEW QUESTION # 43
An infection preventionist is evaluating a new catheter that may decrease the rate of catheter-associated urinary tract infections. Which of the following provides the BEST information to support the selection of this catheter?
- A. Staff member preference and product availability
- B. Product materials and vendor information
- C. Value analysis and information provided by the manufacturer
- D. Cost benefit analysis and safety considerations
Answer: D
Explanation:
The correct answer is D, "Cost benefit analysis and safety considerations," as this provides the best information to support the selection of a new catheter aimed at decreasing the rate of catheter-associated urinary tract infections (CAUTIs). According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, selecting medical devices like catheters for infection prevention involves a comprehensive evaluation that balances efficacy, safety, and economic impact. A cost-benefit analysis assesses the financial implications (e.g., reduced infection rates leading to lower treatment costs) against the cost of the new catheter, while safety considerations ensure the device minimizes patient risk, such as reducing biofilm formation or irritation that contributes to CAUTIs (CBIC Practice Analysis, 2022, Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment). This dual focus provides evidence-based data to justify the catheter's adoption, aligning with the goal of improving patient outcomes and reducing healthcare-associated infections (HAIs).
Option A (staff member preference and product availability) is subjective and logistical rather than evidence- based, making it insufficient for a decision that impacts infection rates. Option B (product materials and vendor information) offers technical details but lacks the broader context of efficacy and cost-effectiveness needed for a comprehensive evaluation. Option C (value analysis and information provided by the manufacturer) includes a structured assessment of value, but it may be biased toward the manufacturer's claims and lacks the independent safety and cost-benefit perspective critical for infection prevention decisions.
The emphasis on cost-benefit analysis and safety considerations reflects CBIC's priority on using data-driven and patient-centered approaches to select interventions that enhance infection control (CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.5 - Use data to guide infection prevention and control strategies). This approach ensures the catheter's selection is supported by robust evidence, optimizing both clinical and economic outcomes in the prevention of CAUTIs.
References: CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.5 - Use data to guide infection prevention and control strategies; Domain III: Infection Prevention and Control, Competency 3.3 - Ensure safe reprocessing of medical equipment.
NEW QUESTION # 44
When preparing an educational session, objectives should be written using clear, precise language to describe what the learner is expected to learn. All of the following are examples of appropriate objective verbs EXCEPT:
- A. compare
- B. know
- C. define
- D. explain
Answer: B
Explanation:
The Certification Study Guide (6th edition) emphasizes that educational objectives must be written using measurable, observable action verbs that clearly define learner outcomes. This principle is grounded in adult learning theory and Bloom's taxonomy, both of which are highlighted in the education and communication sections of the guide. Effective objectives allow educators to evaluate whether learning has occurred by observing or assessing learner performance.
The verb "know" is considered inappropriate because it is vague and not measurable. It does not specify how the learner will demonstrate knowledge, making it impossible to objectively assess whether the objective has been achieved. For this reason, "know" is frequently cited in the study guide as an example of a poorly written objective verb.
In contrast, verbs such as define, compare, and explain are acceptable because they describe specific actions the learner can perform. These verbs allow the instructor to evaluate learning through verbal responses, written assessments, or demonstrations. The study guide stresses that well-written objectives should answer the question: What will the learner be able to do at the end of the session?
This concept is commonly tested on the CIC exam because infection preventionists are expected to design and deliver education effectively. Clear, measurable objectives support competency-based education, documentation of learning outcomes, and program evaluation-all essential components of a successful infection prevention program.
Reference: Certification Study Guide (CBIC/CIC Exam Study Guide), 6th edition, Chapter 8: Education and Research.
NEW QUESTION # 45
On January 31, the nursing staff of a long-term care facility reports that five out of 35 residents have developed high fever, nasal discharge, and a dry cough. The BEST diagnostic tool to determine the causative agent is:
- A. Sputum culture
- B. Nasopharyngeal swab
- C. Legionella serology
- D. Blood culture
Answer: B
Explanation:
The scenario describes a cluster of five out of 35 residents in a long-term care facility developing high fever, nasal discharge, and a dry cough, suggesting a potential respiratory infection outbreak. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes the "Identification of Infectious Disease Processes" and "Surveillance and Epidemiologic Investigation" domains, which require selecting the most appropriate diagnostic tool to identify the causative agent promptly. The Centers for Disease Control and Prevention (CDC) provides guidance on diagnostic approaches for respiratory infections, particularly in congregate settings like long-term care facilities.
Option C, "Nasopharyngeal swab," is the best diagnostic tool in this context. The symptoms-high fever, nasal discharge, and a dry cough-are characteristic of upper respiratory infections, such as influenza, respiratory syncytial virus (RSV), or other viral pathogens common in congregate settings. A nasopharyngeal swab is the gold standard for detecting these agents, as it collects samples from the nasopharynx, where many respiratory viruses replicate. The CDC recommends nasopharyngeal swabs for molecular testing (e.g., PCR) to identify viruses like influenza, RSV, or SARS-CoV-2, especially during outbreak investigations in healthcare facilities. The dry cough and nasal discharge align with upper respiratory involvement, making this sample type more targeted than alternatives. Given the potential for rapid spread among vulnerable residents, early identification via nasopharyngeal swab is critical to guide infection control measures.
Option A, "Blood culture," is less appropriate as the best initial tool. Blood cultures are used to detect systemic bacterial infections (e.g., bacteremia or sepsis), but the symptoms described are more suggestive of a primary respiratory infection rather than a bloodstream infection. While secondary bacteremia could occur, blood cultures are not the first-line diagnostic for this presentation and are more relevant if systemic signs (e.
g., hypotension) worsen. Option B, "Sputum culture," is useful for lower respiratory infections, such as pneumonia, where productive cough and sputum production are prominent. However, the dry cough and nasal discharge indicate an upper respiratory focus, and sputum may be difficult to obtain from elderly residents, reducing its utility here. Option D, "Legionella serology," is specific for diagnosing Legionella pneumophila, which causes Legionnaires' disease, typically presenting with fever, cough, and sometimes gastrointestinal symptoms, often in association with water sources. While possible, the lack of mention of pneumonia or water exposure, combined with the upper respiratory symptoms, makes Legionella serology less likely as the best initial test. Serology also requires time for antibody development, delaying diagnosis compared to direct sampling.
The CBIC Practice Analysis (2022) and CDC guidelines for outbreak management in long-term care facilities (e.g., "Prevention Strategies for Seasonal Influenza in Healthcare Settings," 2018) prioritize rapid respiratory pathogen identification, with nasopharyngeal swabs being the preferred method for viral detection. Given the symptom profile and outbreak context, Option C is the most effective and immediate diagnostic tool to determine the causative agent.
References:
* CBIC Practice Analysis, 2022.
* CDC Prevention Strategies for Seasonal Influenza in Healthcare Settings, 2018.
* CDC Guidelines for the Prevention and Control of Outbreaks in Long-Term Care Facilities, 2015.
NEW QUESTION # 46
Which of the following statements characterizes the proper use of chemical disinfectants?
- A. The label on the solution being used must indicate that it kills all viable micro-organisms.
- B. All items to be processed must be cleaned prior to being submerged in solution.
- C. A chemical indicator must be used with items undergoing high-level disinfection.
- D. The solution should be adaptable for use as an antiseptic.
Answer: B
Explanation:
The proper use of chemical disinfectants is a critical aspect of infection control, as outlined by the Certification Board of Infection Control and Epidemiology (CBIC). Chemical disinfectants are used to eliminate or reduce pathogenic microorganisms on inanimate objects, and their effective application requires adherence to specific protocols to ensure safety and efficacy. Let's evaluate each option based on infection control standards:
* A. All items to be processed must be cleaned prior to being submerged in solution.: This statement is a fundamental principle of disinfectant use. Cleaning (e.g., removing organic material such as blood, tissue, or dirt) is a prerequisite before disinfection because organic matter can inactivate or reduce the effectiveness of chemical disinfectants. The CBIC emphasizes that proper cleaning is the first step in the disinfection process to ensure that disinfectants can reach and kill microorganisms. This step is universally required for all levels of disinfection (low, intermediate, and high), making it a characterizing feature of proper use.
* B. The label on the solution being used must indicate that it kills all viable micro-organisms.: This statement is misleading. No disinfectant can be guaranteed to kill 100% of all viable microorganisms under all conditions, as efficacy depends on factors like contact time, concentration, and the presence of organic material. Disinfectant labels typically indicate the types of microorganisms (e.g., bacteria, viruses, fungi) and the level of disinfection (e.g., high-level, intermediate-level) they are effective against, based on standardized tests (e.g., EPA or FDA guidelines). Claiming that a solution kills all viable microorganisms is unrealistic and not a requirement for proper use; instead, the label must specify the intended use and efficacy, which varies by product.
* C. The solution should be adaptable for use as an antiseptic.: An antiseptic is a chemical agent used on living tissue (e.g., skin) to reduce microbial load, whereas a disinfectant is used on inanimate surfaces.
While some chemicals (e.g., alcohol) can serve both purposes, this is not a requirement for proper disinfectant use. The adaptability of a solution for antiseptic use is irrelevant to its classification or application as a disinfectant, which focuses on environmental or equipment decontamination. This statement does not characterize proper disinfectant use.
* D. A chemical indicator must be used with items undergoing high-level disinfection.: Chemical indicators (e.g., test strips or tapes) are used to verify that the disinfection process has met certain parameters (e.g., concentration or exposure time), particularly in sterilization or high-level disinfection (HLD). While this is a recommended practice for quality assurance in HLD (e.g., with glutaraldehyde or hydrogen peroxide), it is not a universal requirement for all chemical disinfectant use. HLD applies specifically to semi-critical items (e.g., endoscopes), and the need for indicators depends on the protocol and facility standards. This statement is too narrow and specific to characterize the proper use of chemical disinfectants broadly.
The correct answer is A, as cleaning prior to disinfection is a foundational and universally applicable step in the proper use of chemical disinfectants. This aligns with CBIC guidelines, which stress the importance of a clean surface to maximize disinfectant efficacy and prevent infection transmission in healthcare settings.
References:
* CBIC Infection Prevention and Control (IPC) Core Competency Model (updated 2023), Domain IV:
Environment of Care, which mandates cleaning as a prerequisite for effective disinfection.
* CBIC Examination Content Outline, Domain III: Prevention and Control of Infectious Diseases, which includes protocols for the proper use of disinfectants, emphasizing pre-cleaning.
* CDC Guidelines for Disinfection and Sterilization in Healthcare Facilities (2021), which reinforce that cleaning must precede disinfection to ensure efficacy.
NEW QUESTION # 47
The sensitivity of a laboratory test is the proportion of persons:
- A. With the disease who have a positive test.
- B. With the disease who have a negative test.
- C. Without the disease who have a positive test.
- D. Without the disease who have a negative test.
Answer: A
Explanation:
Sensitivity describes how well a test correctly identifies people who truly have the disease. It is the proportion of true positives among all people with the disease-i.e., the probability that the test will be positive when the disease is present. CDC training materials describe sensitivity as the ability of a test to correctly identify the presence of disease and connect it to true positives and false negatives, with the standard formula: Sensitivity = TP / (TP + FN).
Therefore, the correct definition is "with the disease who have a positive test" (Option A). Option B describes false negatives (people who have disease but test negative). Option C describes false positives (people without disease who test positive). Option D corresponds to specificity, which is the proportion of people without the disease who test negative (TN / [TN + FP]).
In infection prevention and control, understanding sensitivity is essential when selecting and interpreting screening or diagnostic tests (e.g., for outbreak investigations or surveillance), because low sensitivity increases missed cases (false negatives), potentially allowing ongoing transmission if cases are not recognized promptly.
NEW QUESTION # 48
Peripherally inserted central catheter (PICC)-associated bloodstream infections (BSIs) have been increasing over the past four months. Which of the following interventions is MOST likely to have contributed to the increase?
- A. Use of a positive pressure device on the PICC
- B. Daily bathing adult intensive care unit patients with chlorhexidine
- C. Use of chlorhexidine skin antisepsis during insertion of the PICC
- D. Replacement of the intravenous administration sets every 72 hours
Answer: D
Explanation:
Peripherally inserted central catheter (PICC)-associated bloodstream infections (BSIs) are a significant concern in healthcare settings, and identifying factors contributing to their increase is critical for infection prevention. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes the
"Surveillance and Epidemiologic Investigation" and "Prevention and Control of Infectious Diseases" domains, which align with the Centers for Disease Control and Prevention (CDC) guidelines for preventing intravascular catheter-related infections. The question asks for the intervention most likely to have contributed to the rise in PICC-associated BSIs over four months, requiring an evaluation of each option based on evidence-based practices.
Option C, "Replacement of the intravenous administration sets every 72 hours," is the most likely contributor to the increase. The CDC's "Guidelines for the Prevention of Intravascular Catheter-Related Infections" (2017) recommend that intravenous administration sets (e.g., tubing for fluids or medications) be replaced no more frequently than every 72-96 hours unless clinically indicated (e.g., contamination or specific therapy requirements). Frequent replacement, such as every 72 hours as a routine practice, can introduce opportunities for contamination during the change process, especially if aseptic technique is not strictly followed. Studies cited in the CDC guidelines, including those by O'Grady et al. (2011), indicate that unnecessary manipulation of catheter systems increases the risk of introducing pathogens, potentially leading to BSIs. A change to a 72- hour replacement schedule, if not previously standard, could explain the observed increase over the past four months.
Option A, "Use of chlorhexidine skin antisepsis during insertion of the PICC," is a recommended practice to reduce BSIs. Chlorhexidine, particularly in a 2% chlorhexidine gluconate with 70% alcohol solution, is the preferred skin antiseptic for catheter insertion due to its broad-spectrum activity and residual effect, as supported by the CDC (2017). This intervention should decrease, not increase, infection rates, making it an unlikely contributor. Option B, "Daily bathing adult intensive care unit patients with chlorhexidine," is another evidence-based strategy to reduce healthcare-associated infections, including BSIs, by decolonizing the skin of pathogens like Staphylococcus aureus. The CDC and SHEA (Society for Healthcare Epidemiology of America) guidelines (2014) endorse chlorhexidine bathing in intensive care units, suggesting it should lower, not raise, BSI rates. Option D, "Use of a positive pressure device on the PICC," aims to prevent catheter occlusion and reduce the need for frequent flushing, which could theoretically decrease infection risk by minimizing manipulation. However, there is no strong evidence linking positive pressure devices to increased BSIs; if improperly used or maintained, they might contribute marginally, but this is less likely than the impact of frequent tubing changes.
The CBIC Practice Analysis (2022) and CDC guidelines highlight that deviations from optimal catheter maintenance practices, such as overly frequent administration set replacements, can increase infection risk.
Given the four-month timeframe and the focus on an intervention's potential negative impact, Option C stands out as the most plausible contributor due to the increased manipulation and contamination risk associated with routine 72-hour replacements.
References:
* CBIC Practice Analysis, 2022.
* CDC Guidelines for the Prevention of Intravascular Catheter-Related Infections, 2017.
* O'Grady, N. P., et al. (2011). Guidelines for the Prevention of Intravascular Catheter-Related Infections. Clinical Infectious Diseases.
* SHEA Compendium, Strategies to Prevent Central Line-Associated Bloodstream Infections, 2014.
NEW QUESTION # 49
Which of the following is the correct collection technique to obtain a laboratory specimen for suspected pertussis?
- A. Sputum culture
- B. Nares culture
- C. Cough plate
- D. Nasopharyngeal culture
Answer: D
NEW QUESTION # 50
A team was created to determine what has contributed to the recent increase in catheter associated urinary tract infections (CAUTIs). What quality tool should the team use?
- A. Gap analysis
- B. Failure mode and effect analysis (FMEA)
- C. Plan, do, study, act (PDSA)
- D. Fishbone diagram
Answer: D
Explanation:
The correct answer is B, "Fishbone diagram," as this is the most appropriate quality tool for the team to use when determining what has contributed to the recent increase in catheter-associated urinary tract infections (CAUTIs). According to the Certification Board of Infection Control and Epidemiology (CBIC) guidelines, the fishbone diagram, also known as an Ishikawa or cause-and-effect diagram, is a structured tool used to identify and categorize potential causes of a problem. In this case, the team needs to explore the root causes of the CAUTI increase, which could include factors such as improper catheter insertion techniques, inadequate maintenance, staff training gaps, or environmental issues (CBIC Practice Analysis, 2022, Domain II:
Surveillance and Epidemiologic Investigation, Competency 2.2 - Analyze surveillance data). The fishbone diagram organizes these causes into categories (e.g., people, process, equipment, environment), facilitating a comprehensive analysis and guiding further investigation or intervention.
Option A (gap analysis) is useful for comparing current performance against a desired standard or benchmark, but it is more suited for identifying deficiencies in existing processes rather than uncovering the specific causes of a recent increase. Option C (plan, do, study, act [PDSA]) is a cyclical quality improvement methodology for testing and implementing changes, which would be relevant after identifying causes and designing interventions, not as the initial tool for root cause analysis. Option D (failure mode and effect analysis [FMEA]) is a proactive risk assessment tool used to predict and mitigate potential failures in a process before they occur, making it less applicable to analyzing an existing increase in CAUTIs.
The use of a fishbone diagram aligns with CBIC's emphasis on using data-driven tools to investigate and address healthcare-associated infections (HAIs) like CAUTIs, supporting the team's goal of pinpointing contributory factors (CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competency 2.3 - Identify risk factors for healthcare-associated infections). This tool's visual and collaborative nature also fosters team engagement, which is essential for effective problem-solving in infection prevention.
References: CBIC Practice Analysis, 2022, Domain II: Surveillance and Epidemiologic Investigation, Competencies 2.2 - Analyze surveillance data, 2.3 - Identify risk factors for healthcare-associated infections.
NEW QUESTION # 51
Which of the following is an essential element of practice when sending biohazardous samples from one location to another?
- A. Electronically log and send via overnight delivery
- B. Ship using triple-containment packaging
- C. Transport by an authorized biohazard transporter
- D. Store in a cooler that is labeled as a health hazard
Answer: B
Explanation:
The safe transport of biohazardous samples, such as infectious agents, clinical specimens, or diagnostic materials, is a critical aspect of infection prevention and control to prevent exposure and environmental contamination. The Certification Board of Infection Control and Epidemiology (CBIC) emphasizes adherence to regulatory and safety standards in the "Prevention and Control of Infectious Diseases" domain, which includes proper handling and shipping of biohazardous materials. The primary guideline governing this practice is the U.S. Department of Transportation (DOT) Hazardous Materials Regulations (HMR) and the International Air Transport Association (IATA) Dangerous Goods Regulations, which align with global biosafety standards.
Option A, "Ship using triple-containment packaging," is the essential element of practice. Triple-containment packaging involves three layers: a primary watertight container holding the sample, a secondary leak-proof container with absorbent material, and an outer rigid packaging (e.g., a box) that meets shipping regulations.
This system ensures that biohazardous materials remain secure during transport, preventing leaks or breaches that could expose handlers or the public. The CDC and WHO endorse this method as a fundamental requirement for shipping Category A (high-risk) and Category B (moderate-risk) infectious substances, making it the cornerstone of safe transport practice.
Option B, "Electronically log and send via overnight delivery," is a useful administrative and logistical step to track shipments and ensure timely delivery, but it is not the essential element. While documentation and rapid delivery are important for maintaining chain of custody and sample integrity, they are secondary to the physical containment provided by triple packaging. Option C, "Transport by an authorized biohazard transporter," is a necessary step to comply with regulations, as only trained and certified transporters can handle biohazardous materials. However, this is contingent on proper packaging; without triple containment, transport authorization alone is insufficient. Option D, "Store in a cooler that is labeled as a health hazard," may be part of preparation (e.g., maintaining sample temperature), but labeling alone does not address the containment or transport safety required during shipment. Coolers are often used, but the focus on labeling as a health hazard is incomplete without the triple-containment structure.
The CBIC Practice Analysis (2022) supports compliance with federal and international shipping regulations, which prioritize triple-containment packaging as the foundational practice to mitigate risks. The CDC's Biosafety in Microbiological and Biomedical Laboratories (BMBL, 6th Edition, 2020) and IATA guidelines further specify that triple packaging is mandatory for all biohazardous shipments, reinforcing Option A as the correct answer.
References:
* CBIC Practice Analysis, 2022.
* CDC Biosafety in Microbiological and Biomedical Laboratories (BMBL), 6th Edition, 2020.
* U.S. DOT Hazardous Materials Regulations (49 CFR Parts 171-180).
* IATA Dangerous Goods Regulations, 2023.
NEW QUESTION # 52
Surgical site infection (SSI) data for the previous quarter reveal the following numbers. The surgeon with the highest infection rate is Doctor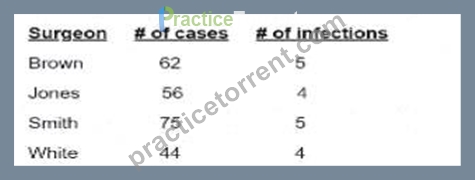
- A. White
- B. Brown
- C. Jones.
- D. Smith
Answer: A
Explanation:
To determinewhich surgeon has the highest surgical site infection (SSI) rate, use the following formula:
A screenshot of a report AI-generated content may be incorrect.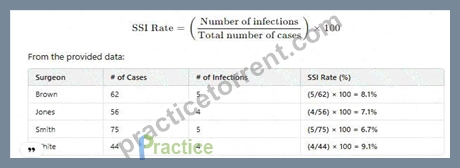
SinceDr. White has the highest SSI rate at 9.1%, the correct answer isD. White.
CBIC Infection Control Reference
SSI rates are calculated usinginfection count per total proceduresand reported aspercentage values.
NEW QUESTION # 53
......
Pass Your Infection Control CIC Exam on May 29, 2026 with 302 Questions: https://actual4test.practicetorrent.com/CIC-practice-exam-torrent.html